Did you know that most cases of thyroid disease are autoimmune in nature? (1)
Hashimoto’s thyroiditis is an autoimmune condition that happens to affect the thyroid gland. This means that our immune system recognizes the thyroid gland as a foreign invader and begins to attack it, eventually leading to the destruction of our thyroid tissue. When this destruction goes on long enough, the person will lose their ability to produce thyroid hormone.
Hashimoto’s is a progressive autoimmune condition that results in the destruction of the thyroid gland and leads to hypothyroidism — and in some cases, to other types of autoimmune conditions as well. (2)
The condition may take many years to develop and is thought to be triggered by damage to the thyroid gland. This results in immune cells congregating in the thyroid gland, and eventually losing their ability to differentiate the thyroid gland from a foreign invader (like a virus or bacteria).
Hashimoto’s is not usually discovered until it has progressed to the advanced stages, where there is significant damage to the thyroid gland.
In this article, I’d like to start at the beginning and walk through the stages of Hashimoto’s. I’ll cover:
- How Hashimoto’s is diagnosed
- The 5 stages of Hashimoto’s
- Reversing the condition
How is Hashimoto’s Diagnosed?
It takes an average of 10 years to be diagnosed with Hashimoto’s between the start of the autoimmune attack on the thyroid gland, and when the person is diagnosed. I had symptoms of thyroid disease for over a decade before I was diagnosed with Hashimoto’s, and many of my clients and readers share a similar timeline between first having symptoms and getting an official diagnosis.
Getting a diagnosis can take so long because most conventional doctors only test one’s TSH levels, but they won’t be elevated until stage 4. There are better tests — that are covered by insurance — that can reveal thyroid disease up to a decade before a change in TSH is detected. But in my experience, most doctors won’t run these tests until a change in TSH is seen. It is really quite backward!
The longer this immune response is in place, the more thyroid damage occurs — and the greater the likelihood of the person progressing to hypothyroidism, where the thyroid gland becomes so damaged that it is no longer able to make enough thyroid hormone.
If we detect the condition earlier, we can prevent the damage…not to mention a decade of symptoms!
The most helpful tests for diagnosing Hashimoto’s include thyroid antibody tests (TPO and TG antibodies) and thyroid ultrasounds. If your doctor won’t order these tests for you, you can self-order them through Ulta Lab Tests, for a relatively low cost. Additionally, some insurance plans will reimburse patients for the labs they order online.
Left unbalanced, the immune system may go on to attack different parts of the body, leading to the development of other autoimmune conditions.
There are no current treatment recommendations or guidelines in the world of conventional medicine to address the immune system attack on the thyroid gland. Rather, the focus is on restoring normal thyroid hormone levels.
In the case when a person is found to have Hashimoto’s with thyroid function that still falls within the normal limits by standard reference ranges, most conventional doctors will say: “I can’t do anything for you now, but follow up with me when your thyroid burns out. We can start you on medications at that point.”
Giving thyroid medications to a thyroid-deficient person is extremely important and can save lives, but this type of “rescue care” does nothing for preventing the progression of the autoimmune condition or for helping a person heal from the condition.
It’s akin to pouring more water into a bucket with a hole in it, without plugging up the leak!
Medications are very important, of course, if someone has a low level of thyroid hormones.
However, they will only address the symptoms — and not the root causes — of the autoimmune disorder.
Hashimoto’s Stages
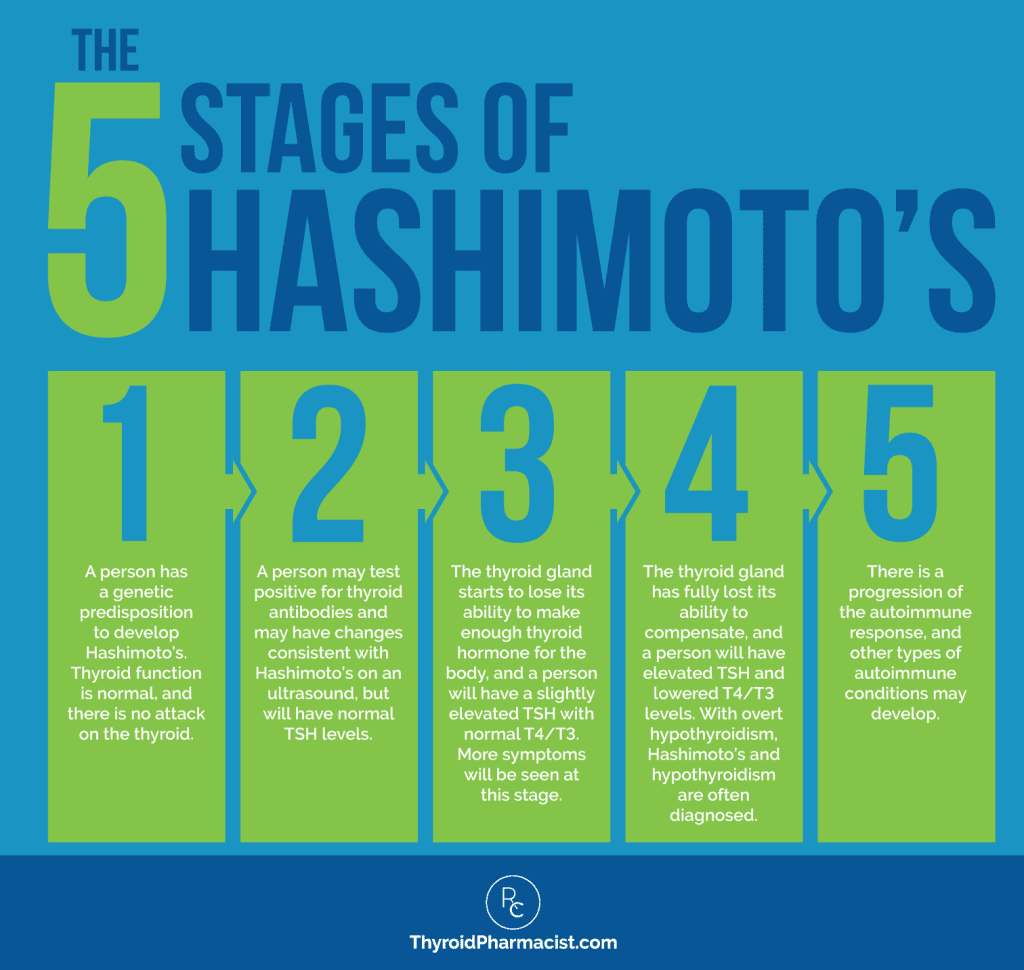
In a 2014 article, Wiersinga and colleagues identified 5 stages of Hashimoto’s. (3)
Stage 1: Genetic Predisposition
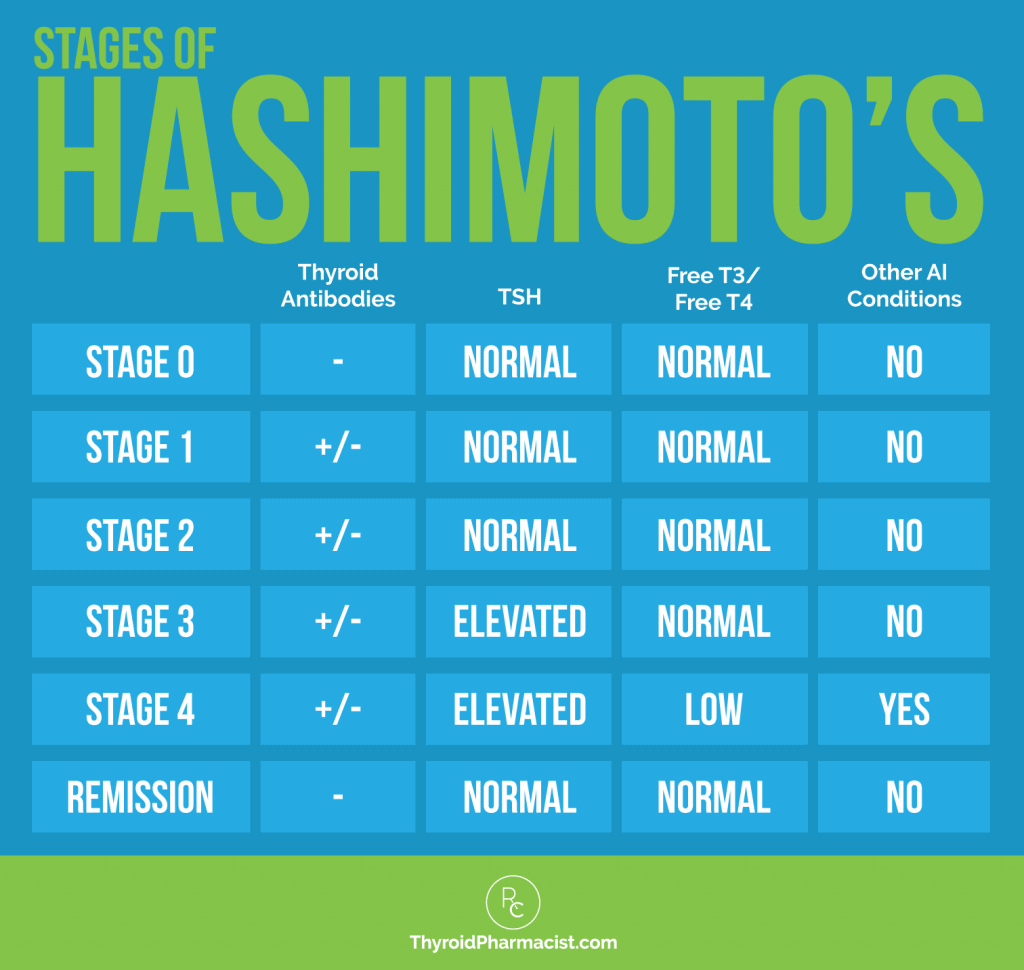
In the initial stage, a person will have the genetic predisposition for Hashimoto’s, but they will not have been exposed to the necessary triggers, and thus will have normal TSH and T4/T3 hormones.
They will not have any thyroid antibodies, nor any changes in their thyroid gland. Alternatively, this could be called stage 0, as there are no manifestations of disease at this point.
If you have thyroid disease, then this may be the stage your relatives and children are currently in. Or, if you have a family member with thyroid disease and you’re reading this, you could be in this stage. This stage is the best time to think about prevention. (4, 5)
For more information on this, I encourage you to check out this article I wrote on preventing Hashimoto’s.
Stage 2: Immune Cell Infiltration of the Thyroid Gland
Hashimoto’s is characterized by an overabundance of lymphocytes (white blood cells) in the thyroid gland. In small amounts, these immune cells play an important cleanup role, but when there are too many of them in an organ, this means trouble. It is thought that, initially, the immune cells may be there with good intentions — to clean up dead and diseased thyroid cells — but at some point, they begin to attack healthy thyroid tissues as well.
In this early stage of Hashimoto’s, a person will usually have elevated thyroid antibodies. Up to 80-90 percent may show an elevation of thyroid antibodies in blood, when tested for thyroglobulin and thyroid peroxidase antibodies, respectively. (6)
However, some people may never have thyroid antibodies present in blood — but sure enough, upon a thyroid ultrasound or biopsy, changes in the gland that are consistent with Hashimoto’s, will be apparent. (7)
This stage may go on for decades before enough damage is done, and before one can detect a change in thyroid hormone levels on a blood test — at this stage, the TSH, Free T3, and Free T4 levels will be normal.
Even in this stage, people may experience symptoms such as anxiety, fatigue, miscarriage/infertility, mood swings, excess weight, or weight loss, because their body is fighting hard to keep their thyroid levels normal, and this can be exhausting and draining on the usual body functions and nutrients.
Additionally, in this stage, there is almost always impaired gut wall function. (8)
Sadly, at this stage, most patients are not diagnosed with Hashimoto’s by conventional medicine. When they are, they’re usually told to wait and watch, and may even be referred to psychiatrists or offered antidepressants for their “mood symptoms.” ?
This is the ideal stage to instill lifestyle interventions and the root cause approach to prevent the progression of the condition and damage to the thyroid gland, as the inflammation in your body has just begun at this point.
In a broad overview, you’ll need to identify your triggers and strengthen your body by addressing:
I’ve had many people reverse their antibodies and symptoms at this stage by just going gluten-free — according to my survey results, 70 percent of participants said their digestive symptoms improved on a gluten-free diet — but some may need a deeper exploration.
I outline my tried and tested protocols for doing all of the above in my book Hashimoto’s Protocol, and you can read more about the importance of finding your root cause in my article.
Can you have no thyroid antibodies but still have Hashimoto’s?
Yes, this is known as seronegative autoimmune thyroiditis, or serum-negative Hashimoto’s.
80-90 percent of people with Hashimoto’s will have TPO antibodies, TG antibodies, or both. (6) However, some people will never test positive for thyroid antibodies, yet may have full-blown Hashimoto’s, with all the symptoms associated with it.
In seronegative Hashimoto’s, the person will still have the hypoechoic pattern on their thyroid gland that is seen with Hashimoto’s upon ultrasound examination. They will also have thyroid autoimmunity, but may not have measurable circulating thyroid antibodies. (9)
Rotondi and colleagues have determined that seronegative autoimmune thyroiditis is a less aggressive form of Hashimoto’s, but nonetheless, the person may still develop hypothyroidism and even progress to other autoimmune conditions, which may or may not have respective positive antibody blood markers (such as seronegative rheumatoid arthritis). (10)
People who do not have thyroid antibodies will likely have smaller thyroid glands and be less likely to have goiters compared to people with Hashimoto’s antibodies.
Serum-negative Hashimoto’s should be treated the same way as serum-positive Hashimoto’s, of course, with the exception of tracking thyroid antibodies. In serum-positive Hashimoto’s, thyroid antibodies can be used as a marker to determine if one has reduced the autoimmune process.
Stage 3: Subclinical Hypothyroidism
The third stage of Hashimoto’s is known as subclinical hypothyroidism.
In this stage, TSH levels may be slightly elevated on blood tests (3-10 mU/L), and the levels of free T3 and free T4 are going to be normal. The person’s thyroid antibodies may be even higher than in stage 2, as increases in TSH can increase the inflammation of the thyroid gland. Some individuals, however, will continue to be antibody negative.
In the world of conventional medicine, this stage is controversial in terms of treatment. Doctors may take a “wait and watch approach,” but if nothing is done, this is the stage where one would begin to experience more symptoms that will eventually progress to overt hypothyroidism.
Some individuals have been able to reverse their condition at this stage without using medications, but I would not linger in this stage for too long, as an elevated TSH contributes to thyroid gland inflammation. Studies have shown that adding a small dose of thyroid medication to lower the TSH at this stage, results in a reduction of thyroid antibodies and can also make a big difference in your symptoms. (11)
While I understand that some people may have a dogma against medications and would prefer to do things the natural way, as a pharmacist, Hashimoto’s patient, and advocate, I am not a proponent of telling my readers to martyr themselves for a cause. In contrast to other medications that act as artificial chemical messengers to block or activate pathways in our bodies, thyroid medications have the same chemical structure as our internally produced thyroid hormones, and most of the symptoms associated with thyroid medications are usually due to improper dosing.
Thus, I, along with most progressive, integrative, and functional medicine physicians, will often recommend thyroid hormone treatment at this stage (some even advocate for treatment with thyroid medications during stage 2).
To learn more about optimizing thyroid medications, download my free eBook below!
In some cases, once the autoimmune attack is balanced, the person may be able to wean off thyroid medications naturally, under their doctor’s supervision.
Lifestyle interventions and the root cause approach are also critical at this stage to feel better, prevent further damage, and reverse the condition!
Stage 4: Overt Hypothyroidism
At this stage, the person has started to have thyroid gland failure. Their thyroid gland will be destroyed to the point where they will no longer be able to make their own thyroid hormone.
The person will have an elevated TSH, with low levels of free T3 and free T4. Thyroid antibodies may be even higher than in previous stages. This is the most common stage when a person is diagnosed, as the person usually has a significant amount of thyroid symptoms at this point.
This is also the stage where a person will require thyroid medications to prevent serious health consequences. Even the staunchest conventional physicians almost always recommend thyroid medication at this point.
Lifestyle changes and the root cause approach are critical at this stage, as you will likely be very symptomatic. Since you will have likely had an inflammatory process in your body for almost a decade at this point, you will need to take on the most aggressive treatment.
I often recommend Low Dose Naltrexone (LDN) at this point to prevent the progression of autoimmunity.
At stage 4, natural tissue regeneration is going to be much more challenging, but luckily, there are new options that exist that can accelerate thyroid tissue repair (see my article about lasers for tissue regeneration to learn about experimental strategies that may help).
Stage 5: Progression to Other Autoimmune Disorders
Having Hashimoto’s puts a person at greater risk for developing other autoimmune conditions like celiac disease, psoriasis, Sjogren’s, rheumatoid arthritis, lupus, multiple sclerosis, and many others… (12-14)
This is a progression of the autoimmune response — as the immune system continues to be imbalanced, it may find additional glands and body tissues to attack, such as the small intestine in celiac disease, the saliva and tear glands in Sjogren’s, and the joints in rheumatoid arthritis. (15)
At this stage, the person will have been likely treated with thyroid medications, so if they are receiving ideal treatment, their TSH, Free T3, and Free T4 numbers should be in a good range.
But, unfortunately, thyroid medications and removing the thyroid gland do nothing to stop the disease progression.
If a person’s hormones are not well-controlled with medications, if they have an enlarged thyroid gland, out-of-control antibodies, Graves’ disease, thyroid nodules, or thyroid cancer, or are not able to have balanced thyroid hormones as they swing from hyper/hypothyroidism, some doctors may recommend surgical removal of the thyroid gland.
Removing the thyroid gland will eliminate thyroid antibodies, but unfortunately, will not stop the autoimmune progression.
Additionally, people who have had their thyroid glands removed (or who have gone through radioactive iodine treatment) may suffer adverse reactions from these procedures and will need to take thyroid medications for the rest of their lives.
That said, it is still possible to reverse autoimmunity and significantly reduce and eliminate the symptoms of other autoimmune conditions.
I recommend the fundamental Hashimoto’s Protocol approach, as well as many advanced protocols at this stage, including LDN, an elimination diet, and treating infections, to help you reverse the autoimmunity.
As long as the thyroid gland has not been completely destroyed, surgically removed, or treated with iodine, there is still some hope for restoring function through advanced protocols like low-level laser therapy. (16)
Depending on how advanced the other autoimmune conditions may have become, the person may need additional organ-specific therapies that are beyond the scope of this article (such as specialized exercises, medications, and whole-body light therapy for multiple sclerosis).
It’s important to note here that autoimmune conditions do not always start with Hashimoto’s. It is thought that the first organ that becomes susceptible to autoimmune damage is the “weakest link,” where the person has a genetic predisposition or the organ has become damaged. (17)
Hashimoto’s is the most common autoimmune condition, but the thyroid gland is not always the “weakest link” for everyone. A person may start off with a different autoimmune condition, like celiac disease, and then progress to Hashimoto’s.
Reversing the Condition
When I was diagnosed with Hashimoto’s, a part of me was relieved. I felt like I had the answer to my many years of symptoms and that, perhaps, thyroid medications would help me feel normal again. But another part of me was confused: if my immune system was out of balance and causing my thyroid problem, why was I not trying to balance my immune system? It seemed foolish.
It reminded me of when I was a kid and my older brother would pick on me. I would complain to my mom, but, tired of her kids’ constant bickering, she told me to “ignore him and he will just go away.”
Of course, ignoring my brother never worked, and eventually, I had to take things into my own hands. Now, while ignoring him didn’t work, fighting certainly didn’t work either — he’s four years older than me, and has the tall genes!
It took some creative, outside-of-the-box thinking, but eventually, I found a way to outsmart him, and he stopped picking on me. I was always a little nerdy, so I offered to do his homework and write his papers for him, in exchange for some peace and respect. The same works for thyroid disease; rather than ignoring the condition or becoming a “thyroid warrior” where we are essentially battling ourselves, we need to think about how to outsmart the condition!
I felt like a little kid in the doctor’s office again, and I wanted to know if there was anything I could do to outsmart my immune system.
Additionally, while my weight, energy levels, and anxiety all improved once I started on thyroid medications, I also had many other symptoms that were not “thyroid related,” per se, and not responsive to thyroid treatment, like my acid reflux, irritable bowel syndrome, joint pain, and fatigue.
I knew that I could not change my genes, but perhaps if I were to find and identify my triggers, I would be able to prevent the progression of the condition.
So I searched for ways to reverse autoimmunity and came across a word that became my goal: remission.
Remission is defined as “the state of absence of disease activity in patients with a chronic illness, with the possibility of the return of disease activity.” While going into remission was not the same as finding a “cure,” I thought it would be a more realistic goal to shoot for.
The remission stage is the point where a person has addressed their underlying triggers and has eliminated them. The person will have a healthy gut and adrenals, be cleared of toxins, have appropriate levels of macro and micronutrients, and will likely have seen a significant drop in their thyroid antibodies.
The goal is to get them <35 IU/mL. (Some people have been able to reduce theirs down to 0 IU/mL!)
While there is no cure for Hashimoto’s, we can put it into remission by eliminating the underlying triggers and thyroid antibodies — and in many cases, we can regenerate and heal thyroid tissues using innovative, experimental therapies.
The Takeaway
Some endocrinologists may say that it’s inappropriate to diagnose a person with Hashimoto’s solely based on the presence of thyroid antibodies (which may be present in 10-20 percent of the general population) if they have a “normal” TSH and do not present with any thyroid symptoms. (18)
However, a 2013 study found that people with thyroid antibodies have similar structural features and blood flow patterns on ultrasound tests, as those with Hashimoto’s who have progressed to overt hypothyroidism. (19) Thus, changes in the thyroid gland may start long before the symptoms of hormonal imbalances finally manifest.
In my opinion, I believe that people should be screened for Hashimoto’s through antibody and/or ultrasound testing. This early detection of the autoimmune process will help a person prevent a myriad of unpleasant symptoms, as well as the progression of the destruction of the thyroid gland, if the root cause of the condition can be identified.
While it’s possible to regenerate thyroid tissue and return to normal thyroid function (even with the normalization of thyroid tissue appearance on ultrasound), it’s obviously much easier to prevent damage than it is to repair it!
By digging for your own personal triggers — which are often food sensitivities, nutrient depletions, toxins, stress, or infections — and addressing gut health, you can often nip the disease in the bud before it reaches a more advanced stage. I’ve seen many people reverse their antibodies in the early stages with simple changes like going gluten free!
It’s my hope that by spreading awareness of Hashimoto’s symptoms, optimal lab ranges (instead of “normal” lab ranges), and empowering people with the knowledge they need to advocate for themselves in the doctor’s office, we can dramatically shorten the average time it takes for Hashimoto’s to be diagnosed.
My book Hashimoto’s Protocol can help you address your Hashimoto’s, regardless of the stage you find yourself in — even if you’ve had your thyroid gland removed! In it, I outline a proven treatment that has helped thousands heal and many others feel better, while reversing the autoimmune damage at the root of the disease.
I’d love to hear your story! At what stage were you diagnosed with Hashimoto’s?
P.S. You can download a free Thyroid Diet Guide, 10 thyroid-friendly recipes, and the Nutrient Depletions and Digestion chapter for free by signing up for my newsletter. You will also receive occasional updates about new research, resources, giveaways, and helpful information.
For future updates, make sure to follow us on Facebook and Instagram too!
References
- Ragusa F, Fallahi P, Elia G, et al. Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best Pract Res Clin Endocrinol Metab. 2019;33(6):101367. doi:10.1016/j.beem.2019.101367
- Mincer DL, Jialal I. Hashimoto Thyroiditis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 28, 2021.
- Wiersinga WM. Thyroid autoimmunity. Endocr Dev. 2014;26:139-157. doi:10.1159/000363161
- Balázs C. Örökletes és környezeti tényezők szerepe autoimmun pajzsmirigybetegségekben [The role of hereditary and environmental factors in autoimmune thyroid diseases]. Orv Hetil. 2012;153(26):1013-1022. doi:10.1556/OH.2012.29370
- Lee HJ, Li CW, Hammerstad SS, Stefan M, Tomer Y. Immunogenetics of autoimmune thyroid diseases: A comprehensive review. J Autoimmun. 2015;64:82-90. doi:10.1016/j.jaut.2015.07.009
- Fröhlich E, Wahl R. Thyroid Autoimmunity: Role of Anti-thyroid Antibodies in Thyroid and Extra-Thyroidal Diseases. Front Immunol. 2017;8:521. Published 2017 May 9. doi:10.3389/fimmu.2017.00521
- Rotondi M, de Martinis L, Coperchini F, et al. Serum negative autoimmune thyroiditis displays a milder clinical picture compared with classic Hashimoto’s thyroiditis. Eur J Endocrinol. 2014;171(1):31-36. doi:10.1530/EJE-14-0147
- Fasano A. All disease begins in the (leaky) gut: role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases. F1000Res. 2020;9:F1000 Faculty Rev-69. Published 2020 Jan 31. doi:10.12688/f1000research.20510.1
- Croce L, De Martinis L, Pinto S, et al. Compared with classic Hashimoto’s thyroiditis, chronic autoimmune serum-negative thyroiditis requires a lower substitution dose of L-thyroxine to correct hypothyroidism – journal of endocrinological investigation. SpringerLink. https://link.springer.com/article/10.1007/s40618-020-01249-x. Published April 21, 2020. Accessed July 19, 2022.
- Rotondi M, de Martinis L, Coperchini F, et al. Serum negative autoimmune thyroiditis displays a milder clinical picture compared with classic Hashimoto’s thyroiditis. Eur J Endocrinol. 2014;171(1):31-36. doi:10.1530/EJE-14-0147
- Adlin V. Subclinical hypothyroidism: deciding when to treat. Am Fam Physician. 1998;57(4):776-780.
- Boccuti V, Perrone A, D’Introno A, Campobasso A, Sangineto M, Sabbà C. An unusual association of three autoimmune disorders: celiac disease, systemic lupus erythematosus and Hashimoto’s thyroiditis. Auto Immun Highlights. 2016;7(1):7. doi:10.1007/s13317-016-0079-9
- Cojocaru M, Cojocaru IM, Silosi I. Multiple autoimmune syndrome. Maedica (Bucur). 2010;5(2):132-134.
- Ruggeri RM, Trimarchi F, Giuffrida G, et al. Autoimmune comorbidities in Hashimoto’s thyroiditis: different patterns of association in adulthood and childhood/adolescence. Eur J Endocrinol. 2017;176(2):133-141. doi:10.1530/EJE-16-0737
- Harpreet S, Deepak J, Kiran B. Multiple autoimmune syndrome with celiac disease. Reumatologia. 2016;54(6):326-329. doi:10.5114/reum.2016.64911
- Höfling DB, Chavantes MC, Juliano AG, et al. Assessment of the effects of low-level laser therapy on the thyroid vascularization of patients with autoimmune hypothyroidism by color Doppler ultrasound. ISRN Endocrinol. 2012;2012:126720. doi:10.5402/2012/126720
- Ludwig RJ, Vanhoorelbeke K, Leypoldt F, et al. Mechanisms of Autoantibody-Induced Pathology. Front Immunol. 2017;8:603. Published 2017 May 31. doi:10.3389/fimmu.2017.00603
- Sinclair D. Thyroid antibodies: which, why, when and who?. Expert Rev Clin Immunol. 2006;2(5):665-669. doi:10.1586/1744666X.2.5.665
- Chaudhary V, Bano S. Thyroid ultrasound. Indian J Endocrinol Metab. 2013;17(2):219-227. doi:10.4103/2230-8210.109667
Note: Originally published in April 2017, this article has been revised and updated for accuracy and thoroughness.


